


Surgeons used a new technique to attach a thought-controlled robot arm directly to an amputee’s stump, giving him a far greater range of motion with the advanced prosthetic limb.
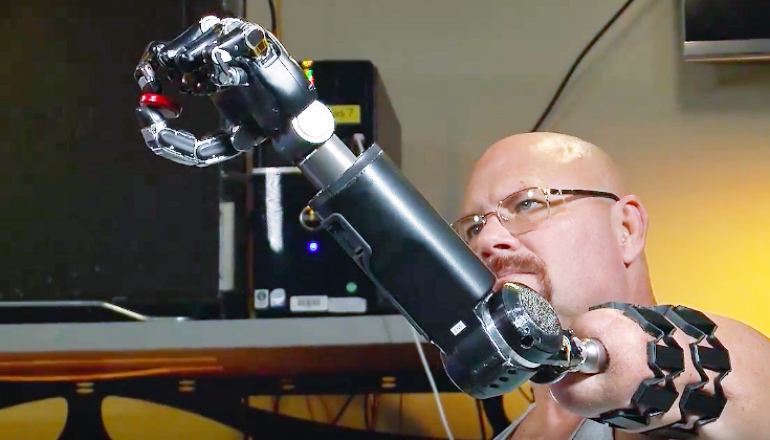
The system, involving an implant inserted into the bone at the end of the residual limb, allows test patient Johnny Matheny to use the arm without the constraining and sometimes uncomfortable harness he previously used when experimenting with the Modular Prosthetic Limb (MPL).
“It’s all natural now,” Metheny says after his first trial run using the MPL with the new implant. “Nothing is holding me down. Before, I had limited range; I couldn’t reach over my head and behind my back. Now—boom!—that limitation is gone.”
Matheny, whose left arm was amputated in 2008 because of cancer, is a pioneer of advanced arm prosthetics. He was the first patient at the Johns Hopkins Hospital to undergo targeted muscle reinnervation, surgery that reassigns the nerves that once controlled the arm or hand.
That surgery is what makes it possible for him to use and control an advanced prosthetic device like the MPL much as a non-amputee would use an arm: the brain send signals through the nerves to direct movement.
The combination in Matheny of both the reinnervation and the implanted connection system is another first for the Revolutionizing Prosthetics program, a Defense Department-funded effort led by the Applied Physics Laboratory. The goal is to provide better functionality for soldiers and for civilian amputees as well.
THE SOCKET IS CRITICAL
“This accomplishment has eliminated one of the biggest gaps in prosthetic development: the socket,” says Michael McLoughlin, chief engineer in APL’s Research and Exploratory Development Department.
The socket—the part of the prosthesis adjacent to the stump—is critical. If it doesn’t fit correctly, the patient can experience pain, sores and blisters, and the prosthesis will feel heavy and cumbersome, says Courtney Moran, a clinical prosthetist who works closely with patients. Even with well-designed sockets, patients have problems with heat, sweating, and chafing, Moran says.
“The [old harness system] does get a little uncomfortable after working with the MPL for a while,” says Matheny, one of several patients who has helped scientists, engineers, and physicians fine tune the prosthetic’s capabilities and test its usability.
When Matheny learned about surgery that would allow him to mount the prosthetic arm directly to his residual limb, he jumped at the chance. The procedure is called osseointegration: First, a threaded titanium implant called a fixture is inserted into the marrow space of the bone in the residual limb. Several weeks later, a titanium extension known as an abutment is attached to the fixture and brought out through the soft tissues and skin. The prosthesis can then be attached to the abutment.
ATTACHING THE DEVICE
Richard McGough, chief of musculoskeletal oncology at the University of Pittsburgh Medical Center, performed the first surgery in March 2015 and the second in June, making Matheny the first US patient with both the TMR and osseointegration. Four months later, he traveled to APL and attached the MPL directly to his body for the first time.
“Before, the only way I could put the prosthetic on was by this harness with suction and straps, but now, with osseointegration, the implant does away with all that,” said Matheny after the MPL was attached.
Over three days, Matheny went through exercises in APL’s prosthetics laboratory to test the limits of his new control and range of motion. Moran and the team had planned to take it slow and easy, she says.
“We were conservative in our expectations,” she adds, “because we wanted to be cautious about how much load we were putting on the implant, how much we were asking him to do, and to make sure that we had a number of safety considerations in place and somewhat temper expectations for him.”
Matheny, however, had done his research and was more than prepared.
“He had configured a weighted attachment for the implant that was about 3 pounds, and he had been doing exercises on his own with this weighted implant, which really put us at a position to do more right from the get-go,” she says.
He was able to demonstrate individual finger control, simultaneous finger control, 2 degrees of freedom at the wrist, and multiple grasps. He also worked through simulated activities of daily living.
Matheny’s achievement “moves the whole field forward, and not just a small step,” McLoughlin says. “The challenge for us next is to really figure out how to get this technology out of the laboratory and into the hands of people that need it.”
Source: Johns Hopkins University and Futurity.org




{kind=link}